
Introduction: When a Child’s Irritability Becomes More Than a Phase
Every child has tough days. Tantrums, backtalk, and mood swings are part of growing up. But what happens when those outbursts happen almost every day, last for over a year, and feel way out of proportion?

That may be something deeper than a phase.
Disruptive mood dysregulation disorder (DMDD) is a childhood condition marked by extreme, ongoing irritability. Kids with DMDD have severe temper outbursts three or more times a week, and they stay angry or irritable most of the day between blow-ups. According to the Disruptive Mood Dysregulation Disorder: The Basics guide from the National Institute of Mental Health, these symptoms must last at least 12 months before a diagnosis is made.
Recognizing DMDD early matters. Without help, the constant conflict can harm school performance, friendships, and family life. But with the right support, many children learn to manage their emotions and build healthier habits.
This article explains what DMDD is, how it differs from typical moodiness, and what steps you can take to help your child. We’ll cover the DSM-5 criteria, treatment options, and practical tips for parents and caregivers.
Because mental health terms carry weight, it’s important to Use Labels Carefully. DMDD is a real condition, but not every irritable child has it. Understanding the difference is the first step toward getting the right help.
For a closer look at the signs, you can read our guide on disruptive mood dysregulation disorder how to spot the signs and help your child.
What Is Disruptive Mood Dysregulation Disorder?
So what exactly is disruptive mood dysregulation disorder? Think of it as a diagnosis that exists to catch something the mental health field used to miss: kids who are chronically, severely irritable without clear cause.
Before 2013, many of these children were incorrectly diagnosed with bipolar disorder or just labeled "difficult." That changed when DMDD was added to the DSM-5. According to the DSM-5 criteria for DMDD overview, the diagnosis can only be made in children aged 6 to 18, and symptoms must start before age 10.
That age cutoff is important. DMDD is not something that suddenly appears in a teenager who was calm as a younger child. The pattern of explosive anger and persistent irritability has to be present from early childhood.
Here’s the thing that separates DMDD from normal moodiness. Every kid gets grumpy. But DMDD is a chronic condition that causes real problems at home, at school, and with friends. A child with DMDD might spend most of their day feeling angry or tense, even when nothing bad is happening. Then three or more times a week, they explode into verbal or physical outbursts that seem completely out of proportion.
This pattern lasts for at least 12 months. And during that year, there is no break of three months or more without symptoms.
If you are wondering how DMDD fits alongside other mental health categories, it belongs to the depressive disorders section in the DSM-5. That means it is considered a mood disorder, not a behavior problem. The core issue is emotional dysregulation, not defiance.
Understanding this distinction matters because the right treatment starts with the right label. A child who is simply labeled "angry" may not get the support they actually need. For a broader look at how different mental health conditions are classified and treated, check out this guide on clinical mental health counseling for modern practitioners.
In short, DMDD is a real, diagnosable condition that requires a specific approach. It is not just bad behavior or a phase your child will outgrow on their own.
DSM-5 Diagnostic Criteria: A Closer Look
To properly diagnose disruptive mood dysregulation disorder, professionals turn to the DSM-5. This manual lays out specific rules that separate DMDD from other conditions.
Let’s break down the exact criteria.
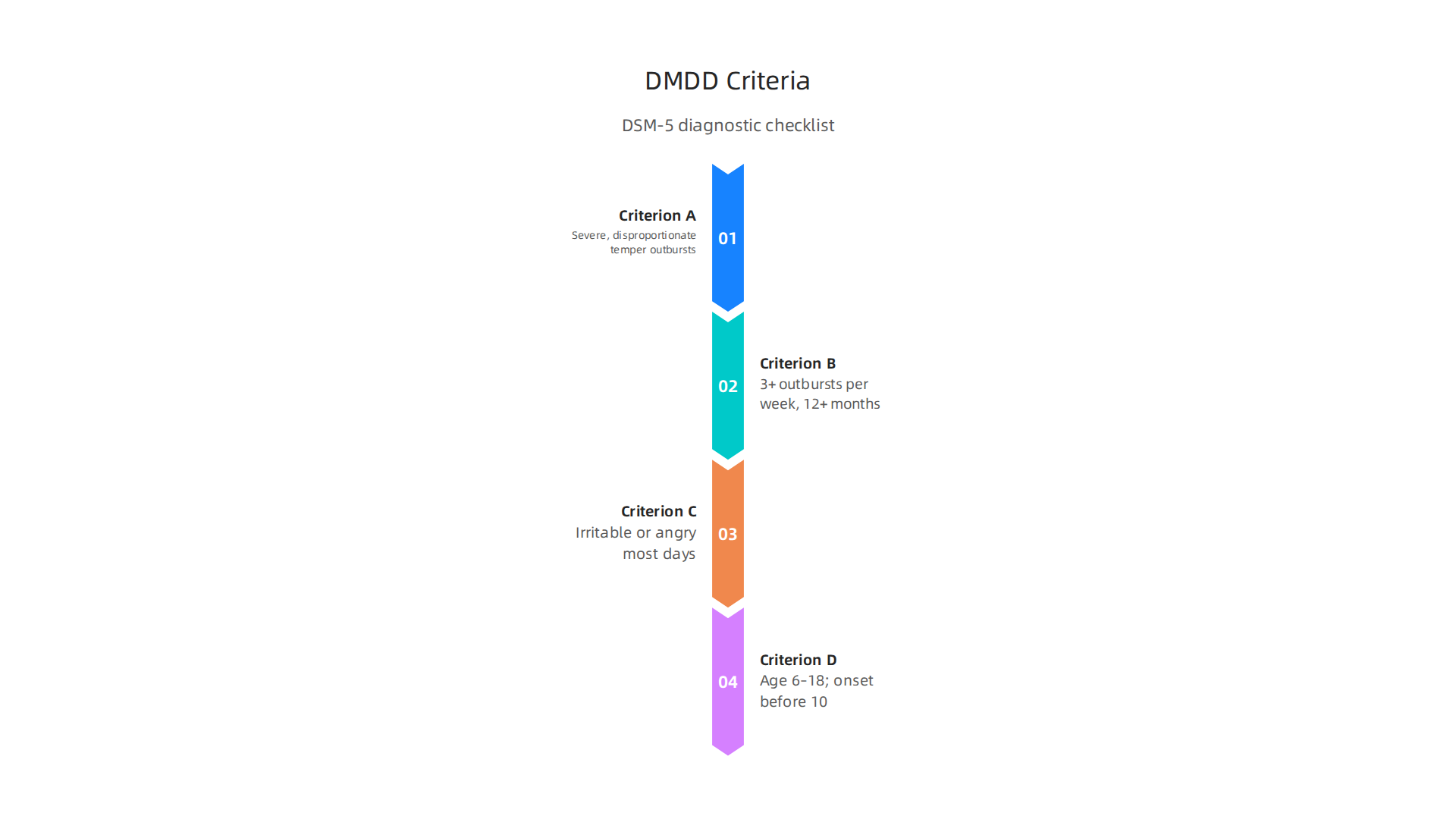
Criterion A focuses on severe temper outbursts. These are not normal tantrums. They are verbal explosions like screaming or yelling, and often behavioral ones like hitting, breaking things, or hurting others. The key detail is that the outbursts are grossly out of proportion to what caused them. A spilled glass of milk might trigger a full meltdown that lasts 30 minutes.
Criterion B says these outbursts happen three or more times per week on average. And they keep happening for at least 12 months. According to the NIMH overview of DMDD basics, the child must show this pattern consistently without a break of three months or longer.
Criterion C covers the mood between outbursts. The child is persistently irritable or angry most of the day, nearly every day. They may seem grumpy, tense, or on edge even during calm moments. This is what makes DMDD different from occasional blowups.
Criterion D sets the age rules. The diagnosis cannot be made before age 6 or after age 18. And symptoms must start before age 10. This means you cannot diagnose DMDD in a teenager who suddenly becomes irritable. The pattern has to be there from early childhood.
If you want to compare DMDD with other behavioral conditions, check out this guide on how to spot the signs of DMDD in children. It helps you understand what to look for at home.
Mental health terms need real context. That is why it matters to Use Labels Carefully when talking about your child’s behavior. The right label leads to the right help.
DMDD vs. Bipolar Disorder vs. ODD: Getting the Diagnosis Right
One of the trickiest parts of diagnosing disruptive mood dysregulation disorder is that it shares a lot of the same features as other childhood conditions.
Irritability, outbursts, and defiance show up in several different disorders. But the root cause of those behaviors is not the same. Getting the right diagnosis changes everything for your child.

DMDD vs. Childhood Bipolar Disorder
Many kids with DMDD are first told they have bipolar disorder. That is because both conditions involve severe irritability and explosive anger. But there is one major difference: bipolar disorder comes in episodes. A child with bipolar disorder might be manic for a few days or weeks, then feel normal for a while. With DMDD, the irritability never really goes away. It is there almost every day, all day long. This guide on DMDD in children vs. childhood bipolar explains that manic episodes involve distinct periods of elevated mood, increased energy, and grand plans. DMDD does not have those highs. The mood stays grumpy and on edge constantly.
DMDD vs. Oppositional Defiant Disorder (ODD)
ODD is another common mix-up. Kids with ODD refuse to follow rules, argue with adults, and blame others for their mistakes. They do these things on purpose to get what they want or to avoid what they do not like. Their defiance is goal directed. DMDD outbursts are different. They are reactive and completely out of proportion to the situation. A child with DMDD does not plan a meltdown. It just happens. They cannot control it. This breakdown of DMDD vs. ODD highlights that the core mood in DMDD is chronic irritability, while ODD is more about oppositional behavior and argumentativeness.
Why Accurate Diagnosis Matters
Mistaking DMDD for bipolar disorder can lead to unnecessary medications like mood stabilizers or antipsychotics that may not help. Mistaking it for ODD can mean the child gets punished when they really need therapy. The right label leads to the right treatment. If you want to learn more about what to watch for at home, read this guide on how to spot DMDD signs in children.
Mental health terms need real context. That is why it matters to Use Labels Carefully when talking about your child’s behavior. The right label leads to the right help.
Causes and Risk Factors: What Leads to DMDD?
You might wonder why your child has such a hard time controlling their temper while other kids seem fine. The truth is, disruptive mood dysregulation disorder does not have one single cause. Research points to a mix of genetic, brain, and environmental factors working together.
Genetics and Family History
Children with a family history of mood disorders are more likely to develop DMDD. If a parent or sibling has dealt with depression, anxiety, or bipolar disorder, the risk goes up. This does not mean your child is doomed. It just means they may have a genetic vulnerability that makes them more sensitive to stress and frustration.
Brain Differences
Neuroimaging studies show that kids with DMDD have real differences in how their brains process emotions. Parts of the brain involved in attention and impulse control, like the parietal cortex and inferior frontal gyrus, work differently in these children. Researchers are still learning exactly how these differences lead to chronic irritability. For more detail, check out this research on brain function in DMDD from the National Center for Biotechnology Information. The amygdala, which handles threat detection, and the prefrontal cortex, which helps with self control, are also affected. These brain changes make it much harder for a child to calm down once they get upset.
Environmental Stressors
What happens at home matters too. Trauma, inconsistent parenting, and high conflict in the family are all linked to higher rates of DMDD. When a child grows up in an unpredictable environment, their nervous system stays on high alert. That constant state of alarm can come out as explosive anger. The good news is that these environmental factors can be changed with the right support.
The Role of Emotion Regulation and Reward Processing
Underneath all the outbursts, kids with DMDD have trouble managing their emotions and responding to rewards. Their brain struggles to shift attention away from something frustrating. That is why a small disappointment can feel like a crisis. Understanding how reward processing works in the brain can help explain some of the irritability seen in DMDD. For a deeper look at the behavioral mechanisms behind motivation and emotion, you can read the peer white paper The Science of Gamification.
If you want to learn more about what DMDD looks like day to day, visit this guide on how to spot the signs of DMDD and help your child.
Evidence-Based Treatments for DMDD
Once you know the signs, the next step is finding the right treatment. The good news is that disruptive mood dysregulation disorder responds well to a mix of therapies and, in some cases, medication.

The best approach is always tailored to your child’s age, symptoms, and family situation.
Psychotherapy Comes First
Talk therapy is the foundation of DMDD treatment. Cognitive-behavioral therapy (CBT) is one of the most effective options. It helps children learn to spot the thoughts that trigger their anger and replace them with calmer responses. For a deeper look at how this works, see this overview of cognitive behavioral therapy. Dialectical behavior therapy (DBT), adapted for teens, also works well. It teaches skills for handling intense emotions without exploding.
Parent management training is another key piece. Parents learn how to respond to outbursts in ways that reduce conflict and encourage better behavior. Consistency at home makes a huge difference.
When Medication Might Help
For severe irritability or aggression, doctors sometimes add medication. Stimulants can help if your child also has ADHD. Antidepressants or atypical antipsychotics may be used too, but always with caution. The Cleveland Clinic explains that medication is often combined with therapy, not used alone. A healthcare provider should monitor any medication closely.
A Multimodal Approach Works Best
No single treatment does it all. The best results come from combining individual therapy, parent training, school support, and sometimes medication. Your child’s plan should fit their unique needs. If you are trying to tell the difference between various conditions, a mental illness quiz can help you sort out whether symptoms point to DMDD or something like a dissociative disorder. Understanding the difference between psychiatric disorder vs mental illness can also guide your conversations with a professional.
Every child deserves a path forward. With the right support, explosive anger can become manageable, and your family can find peace again.
How to Help Your Child at Home: Practical Parenting Strategies
Professional therapy matters a lot, but what happens in your living room every day can make or break the progress. The way you respond to outbursts, structure your day, and care for yourself all shapes how your child learns to manage their emotions.

Build a Predictable Routine
Kids with DMDD do best when they know what to expect. A predictable daily schedule reduces the anxiety that often triggers explosive anger. Set regular times for meals, homework, play, and bedtime. Stick to them as much as possible. When changes happen, give your child a heads up well in advance.
Clear consequences also help. Your child needs to know exactly what will happen if they break a rule. Keep consequences calm and consistent. For a deeper look at how to handle discipline at home, check out these discipline strategies for children with DMDD from Avery’s House.
Use Simple Techniques in the Moment
Two powerful tools are planned ignoring and labeled praise. Planned ignoring means you do not react to minor annoying behaviors like whining or stomping. This teaches your child that those actions do not get attention. Labeled praise is the opposite. When your child does something good, say exactly what you liked. For example, "I love how you took a deep breath instead of yelling."
Emotion coaching is another win. When your child is upset, name the emotion for them. "I can see you are really angry right now." This helps them connect feelings to words instead of actions.
The CDC offers excellent parent training in behavior management that teaches these skills step by step. Many programs report a parent management training with a 92% success rate when families commit to the methods.
Take Care of Yourself First
Here is a hard truth. Your child’s behavior will drain you. If you are exhausted, frustrated, or isolated, you cannot stay calm enough to use these techniques well. That is why parent self-care is not optional.
Join a support group for parents of kids with DMDD. Talk to a therapist for yourself. Make time for sleep and exercise. When you feel steady, your whole home feels safer for your child. To learn more about how different therapy approaches can help you as a parent, read this guide on perspectives in counseling.
You are not alone in this. Small changes at home, repeated every day, really do add up to a calmer, more connected family life.
Long-Term Outcomes and Prognosis
When you are in the middle of daily meltdowns and constant irritability, it is hard to picture what your child’s future looks like. But you probably wonder about it anyway. Will they grow out of this? What happens when they become a teenager or a young adult?
Research on long-term outcomes gives us both sobering news and real reasons to hope.
Children with disruptive mood dysregulation disorder face a higher risk of developing depression and anxiety disorders as they get older. One major study on the adult diagnostic and functional outcomes of DMDD found that these children were more likely to struggle with mood and anxiety problems in young adulthood. Another report on the long-term prognosis for youth with DMDD confirmed that young adults who had DMDD as children were significantly more likely to be anxious and depressed.
Here is the thing. DMDD itself does not carry over into adulthood as a formal diagnosis. The condition is considered a childhood disorder. But the risks do carry over. Kids with DMDD often grow up to face depression, anxiety, and other challenges.
The good news is that early intervention changes the trajectory. When children get the right help early, many see a real reduction in irritability over time. The symptoms often shift. Teens and young adults may have fewer tantrums but still struggle with internal emotions like sadness or worry.
That is why continued support matters. Even as your child grows, they may need help with emotion regulation and social skills well into young adulthood. Therapy, strong family support, and good habits at home all build the foundation for a healthier future.
If you want to learn more about what DMDD looks like day to day, check out this guide on how to spot the signs of DMDD and help your child.
And remember, mental health terms like disruptive mood dysregulation disorder need real context to be useful. Use Labels Carefully when talking about these conditions so you stay grounded in what they actually mean for your family.
When to Seek Professional Help
Knowing the long-term outlook is helpful, but you might be wondering right now: When is it time to call a doctor? It is not always easy to tell the difference between a difficult phase and something that needs professional support. But there are clear signs that say it is time.
If the outbursts cause major distress for your child or your family, that is a big clue.

If they lead to school suspension or get in the way of normal daily life, you should not wait. A full evaluation can give you answers and a path forward. According to the DMDD diagnosis and treatment guide from Cleveland Clinic, healthcare providers recommend treatment when symptoms are frequent and severe enough to interfere with school, friendships, or home life.
Some red flags mean you need help right away. Self-harm, aggression toward others, or any mention of suicidal thoughts must be taken seriously. These are emergencies. If you see any of these, seek immediate help.
The good news is that many professionals are trained to help with disruptive mood dysregulation disorder. Your child’s primary care provider can start the process. Child psychiatrists and licensed therapists can do a deeper evaluation and coordinate care. Therapy options like cognitive behavioral therapy are often the first step. Learn more with this cognitive behavioral therapy overview to understand how it can teach your child new coping skills.
You do not have to figure this out alone. Getting a professional opinion early can change everything. It gives your child the best chance to learn emotion regulation and feel better over time.
Summary
This article explains disruptive mood dysregulation disorder (DMDD), a childhood mood disorder marked by chronic irritability and severe temper outbursts that occur three or more times per week for at least 12 months and begin before age 10. It walks through the DSM‑5 diagnostic criteria, how to tell DMDD apart from bipolar disorder and oppositional defiant disorder, and the interplay of genetic, brain, and environmental risk factors. The piece outlines evidence‑based treatments—especially psychotherapy like CBT and parent management training—when medication may be used, and practical, day‑to‑day parenting strategies that reduce conflict and build emotional skills. You’ll also learn when to seek professional help, what to expect for long‑term outcomes, and how early intervention can change a child’s trajectory toward better emotional regulation and family functioning.




